68 causes of T wave, ST segment abnormalities BySteven Lome, DO
How often do you see an ECG that is just a little off? Maybe the T wave is flat, oddly-shaped or inverted. Maybe the ST segment is coved, very minimally-depressed or shows some J point elevation.
These are referred to as “non-specific” T wave and ST segment changes on the ECG because they are simply not specifically signaling any medical condition. Here, we consider the potentially-underlying reasons for these annoying minimal ECG changes and explore various clinical situations that could cause T waves and ST segments to deviate from normal.
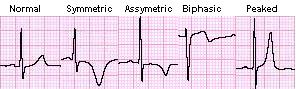
In some instances, T wave changes might suggest specific conditions, such as peaked T waves in hyperkalemia or symmetric T wave inversions during myocardial ischemia. But what about all the other T wave abnormalities, such as flat T waves, biphasic T waves or asymmetric T wave inversions?
Enlarge
Similarly, ST segment abnormalities on the ECG can sometimes be due to a specific cause, such as ST segment elevation myocardial infarction, pericarditis or myocardial ischemia. Other times, there are just subtle abnormalities.
Review the following ECG findings when the ST segment change or T wave change is actually indicative of a specific condition. These are very important not to misinterpret.
ST Segment Elevation MI
Pericarditis
Hyperkalemia
After reading the list below in entirety, you will completely understand why the T wave and ST segment changes mentioned above are sometimes called non-specific. Although some in their severe form have a more classic ECG appearance that could help pinpoint a diagnosis, every situation is different. A mild abnormality (i.e. mild hyperkalemia or a very small MI) may only show a mild ECG change and not a full-blown abnormal finding. When a finding may sometimes be classic, it is listed next to the cause.
VERY early myocardial injury (classic is “hyperacute T waves”)
Reciprocal ischemic changes
Left ventricular aneurysm (classic is persistent ST segment elevation 6 weeks after MI)
Coronary spasm
Digoxin
Quinidine
Tricyclic antidepressants (T-wave changes; classic is QRS widening)
Many medication overdoses (see the below example of a clonidine overdose; this case looked like hyperacute T waves) Enlarge
Atrial flutter (flutter waves overlapping T waves)
Infiltrative cardiomyopathy
Takotsubo cardiomyopathy
Hypertrophic obstructive cardiomyopathy
Apical hypertrophic cardiomyopathy
Arrhythmogenic right ventricular dysplasia
Brugada syndrome
Long QT syndromes
LVH with strain
RVH with strain
Stage 3 pericarditis (T waves flattened)
Cocaine toxicity
Cardiac tumor
Loeffler’s endocarditis
Hypothemia
Mitral valve prolapse
Pericardial effusion
Pericardial abscess
Subarachnoid hemorrhage (deep inverted T waves, QT prolonged as well)
Subdural hematoma (deep inverted T waves, QT prolonged as well)
Intracranial hemorrhage (deep inverted T waves, QT prolonged as well)
Stroke (deep inverted T waves, QT prolonged as well)
Post carotid endarterectomy (deep inverted T waves, QT prolonged as well)
Hyperventilation (can cause ST depression)
Limb lead reversal
ECG lead misplacement
Physiologic junctional depression (occurs with sinus tachycardia)
Pseudo ST-depression (wandering baseline from artifact, poor skin-electrode contact)
Heightened adrenergic state (pain, panic attack, etc...)
Early repolarization
Hypothyroidism
Truncal vagotomy
Hypopituitarism
Gallbladder disease
Adrenal insufficiency
Pulmonary embolism
Post-prandial
Persistent juvenile T-wave pattern
Left-sided pleural effusion
Normal variant
Every time you see an ECG with a T wave or ST segment that is not normal, use this list to identify the possible causes. There are likely additional scenarios I did not think to mention here; please use the comment section to add to the list.