How To Start An IV | Health And Willness
Maybe your like
This post (how to start an IV) may contain affiliate links, which means I get a commission if you decide to purchase through my links, at no cost to you. Please read affiliate disclosure for more information
Learning how to start an IV is a very important skill that every nurse needs to know. Inpatient and ER nurses deal with IVs every day – whether they are inserting them, removing them, or administering fluids or medications through them. If you are new to nursing, then you will need to learn how to insert an IV with confidence and knowledge!

When to start an IV?
The short answer to this is “when an IV is ordered”. However, it is important to critically think as a nurse, and anticipate what will need to be done. Especially as an ER nurse, you may see your patient before the Provider and can start placing an IV if indicated.
If you work as an inpatient nurse, most patients should have at least an IV, midlines, PICC lines, or other central access. These IVs often go bad, and you will need to know how to start an IV in these settings as well.
INDICATIONS to Start an IV:

IV FLUIDS OR MEDS
IV fluids or medications is the main reason an order will be placed to start an IV.
DIAGNOSTIC IMAGING
CTs or MRIs often require an IV for IV contrast to help visualize the anatomy, vasculature, and any potential abnormality going on.

INPATIENT ADMISSION
Most facilities will require an IV be placed if the patient is being admitted. However, the patient can refuse this.
Table of Contents
- When to Start an IV?
- Contraindications to an IV
- Which Gauge to pick?
- IV Equipment
- IV Insertion Procedure
- IV Removal Procedure
When to NOT start an IV?
Contraindications to starting an IV:
There is no outright contraindication to placing an IV, but certain factors will exclude specific locations. These include extremities with:
FISTULAS/GRAFTS
Dialysis patients may have AV fistulas or grafts. You should NOT start an IV in these limbs unless specifically allowed.

MASTECTOMY
Patients with a history of mastectomy or lymph node dissection should not have IVs placed on that side if possible. This can cause/worsen lymphedema.
BLOOD CLOTS
Patient’s with an Active DVT in their arm should not have IVs placed in the same arm – this can further cause irritation of the veins and worsen thrombi formation.
BURNS OR EDEMA
Significant burns or edema should not have an IV placed if possible over the burnt or edematous area.

INFECTION
Do not place an IV overlying an infection like cellulitis. This can introduce bacteria into the blood and lead to sepsis.
It may be best to avoid limbs with significant motor or sensory deficits, as there is unclear evidence that may suggest increased DVT in these extremities. If their arm is numb, they also may not feel when it is infiltrated.
What IV Gauge should you use?
The IV gauge will determine how big the actual needle and catheter are.
The bigger the IV – the faster fluid can be administered. Unfortunately, bigger sizes are also more painful and usually more difficult to start an IV. Bigger IVs also come with an increased risk of phlebitis and can cause some serious irritation to the vein.
24 GAUGE: THE BABY NEEDLE
These are typically used for babies and generally should be avoided in adults. They are very short, flimsy, and won’t last long.
- Good for: Infants
- Bad for: Most other scenarios
22 GAUGE: THE SAFE CHOICE
This is used for many kids and adults, especially older adults with fragile “easily-blown” veins. These are usually OK for IV contrast dye as well, but not for CTA. These are also generally easier to place.
- Good for: Peds, many Med-Surg adult patients, easily blown veins
- OK for: IV contrast, blood return
- Bad for: Massive trauma or fluid resuscitation needs, CT Angiography
20 GAUGE: THE ONE-SIZE-FITS-ALL
20g IVs are an ER nurse’s best friend when you have to start an IV. This is because a 20g IV is adequate for multiple fluid boluses, IV medication infusions, and most CTA requirements. They often give great blood return and labs can often be drawn without hemolysis.
- Good for: Most adult patients, CT Angiography
- OK for: Emergency situations (code blues, RRTs)
- Bad for: Massive trauma or fluid resuscitation needs
18 GAUGE: THE BIG DADDY
18g IVs are your standard “large bore” IV. These are great in critical situations as they provide for rapid administration of fluids or blood products, rapid infusion of critical medications. The down-side is they tend to be a little more difficult to place in the absence of large veins.
- Good for: Critical or emergency situations, rapid fluid administration, CTA, severe sepsis, burns, acute MI, etc
- Bad for: Small, fragile veins
14-16G: THE MONSTERS
The 16g and 14g IVs are very large, and unnecessary for most indications. However, in critical situations these may serve you well.
Also Check out: “10 IV Insertion Tips for Nurses”
Start an IV Clinical Note
Some nurses may tell you to place the largest IV catheter that the vein can support. However, this is contrary to good nursing judgment. If you ask my friend Brian (@TheIVGuy), he will tell you that you should choose your size based on the appropriate ordered therapy and anticipated needs. This means that for most patients, a 20-22 gauge is likely the best and safest choice.
What Equipment to Start an IV?
Before learning how to start an IV, you need to first know which equipment you will need. This becomes like second nature, but when starting out as a new nurse, this is often important to memorize. For an IV insertion, you will need:

IV INSERTION KIT
These kits should include:
- Chlorhexadine or alcohol swab
- Tegaderm dressing
- 2×2 gauze
- Tourniquet
- Tape
IV CATHETER
Your IV catheter of choice, usually 18-22g.
VACUTAINER
A blood transfer device will be needed if you are planning on drawing blood directly you start an IV.
EXTENSION LOOP OR CAP
You will need to place an IV cap or extension loop onto the IV after insertion.

SALINE FLUSH
Make sure you have one or two flushes on hand.
Once you have your equipment, you are ready to know how to start an IV.
How to Start an IV
-
PREPARE THE PATIENT to Start an IV
To start an IV, you will first want to wash your hands (always the right starting point). You will also want to use universal precautions, so put on a pair of clean gloves as you will be possibly interacting with the patient’s blood.
You should already have an idea of where you are going to place the IV and which size IV catheter you are going to use.
 Place the tourniquet on the patient’s arm proximal to the area of cannulation. Look for straight, large veins. Palpate them as veins may not always be visible but can still be felt. Strong veins will have a good amount of bounce to them.
Place the tourniquet on the patient’s arm proximal to the area of cannulation. Look for straight, large veins. Palpate them as veins may not always be visible but can still be felt. Strong veins will have a good amount of bounce to them.Once you are happy with your vein selection, you can start prepping your area. Use a chlorhexidine (CHG) or alcohol swab to gently clean the surrounding area for 30 seconds, and allow it to completely dry. Start with the center and move outward in a circular fashion with alcohol, while CHG requires a back and forth scrubbing action.
With deeper non-visible veins, some nurses will also apply alcohol to a finger of their non-dominant hand to help palpate during the procedure without “contaminating” the site. Please note that this is not the best practice for infection control. You should never tear off the finger of your glove either, instead – learn to palpate with your gloves on.
-
PREPARE YOUR IV KIT
While your site is drying, open your 10cc flush and your extension loop and/or cap.
If you are drawing blood, hook up the blood transfer device to the dry extension loop or cap. Otherwise, you can connect the flush and prime the loop or cap. Set this aside back into your kit to keep it clean.
Open up your IV, take off the needle cap, and twist the end of the catheter to make sure it is loose and ready for cannulation.
-
HOLD SKIN TAUT when you start an IV
Hold the patient’s skin taut with your non-dominant hand to secure the vein underneath, stabilizing it from rolling, and smoothing the skin for insertion.

-
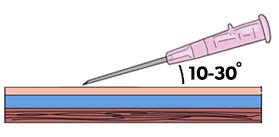
PLAN THE RIGHT ANGLE
Place the tip of the needle against the skin at a 10-30 degree angle when you start an IV. The deeper the vein, the more angular your approach will need to be.

-
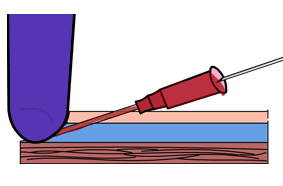
INSERT THE NEEDLE
With the bevel up, puncture the skin and advance through to the vein.
If done correctly, you should see a flashback of blood in the flash chamber and/or catheter. This location will depend on the brand and size of the specific IV catheter. Once a flashback is seen, lower the angle even more parallel with the skin, and advance the whole unit about 2-6mm.

 Place the tourniquet on the patient’s arm proximal to the area of cannulation. Look for straight, large veins. Palpate them as veins may not always be visible but can still be felt. Strong veins will have a good amount of bounce to them.
Place the tourniquet on the patient’s arm proximal to the area of cannulation. Look for straight, large veins. Palpate them as veins may not always be visible but can still be felt. Strong veins will have a good amount of bounce to them.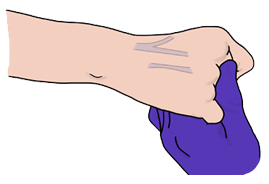

Clinical Note
If you initially don’t see flash of blood, pull the needle and catheter both out almost completely (but do not leave the epidermis). Re-palpate the vein, adjust your angle and advance again. This is termed “digging” and some patients will not tolerate this well. However, oftentimes it may only take 2 or 3 “digs” until success.
-
ADVANCE CATHETER ONLY
Now advance only the catheter forward, sliding it off of the needle and cannulating the vein. If done correctly, the catheter should easily slip into the vein without resistance. If there is dimpling of the skin, the IV is likely within the extravascular space.

-
HOLD PRESSURE AND RETRACT
Before pressing the activation button to retract the needle – take off the tourniquet and apply digital pressure beyond the catheter tip.
Some brands will have a septum or shield function with gauges 20-24, which prevents the backflow of blood and negates the need for venous compression.
Press your activation button to retract the needle.

-
DRAW BLOOD After you Start an IV
If ordered, now is the point where you will draw your blood. Hook up your loop/cap with the blood transfer device to the IV hub.
Draw your blood tubes, and flush with a 10cc pulse flush afterward.If blood is ordered, you can immediately draw this after placing a new IV. If you are not drawing blood, skip this step and instead just connect the primed cap or extension loop to the IV and flush.
After flushing a few mLs, make sure you can pull back blood return. This is reassurance that the IV is in the correct place after you start an IV. Then pulse flush the remaining amount through.
-
SECURE THE IV
Secure the IV with a securement device or tape, and a dressing like Tegaderm. Make sure the insertion site is covered. If you used an extension loop, secure the loop with tape as this can easily get caught on something and pull out the IV.
If the patient is confused or may try pulling the IV out, wrap the IV with Coban, only leaving the cap accessible.
Administer any medications or fluids through the IV as ordered. and Viola – you can check “Start an IV” off your task list!

How to REMOVE an IV
Knowing how to start an IV is important, but you also need to know how to remove an IV! If the patient is discharged or if there is a compilation with the IV, it will need to be removed. Removing the IV is easier, and can be performed by a nurse or a patient care assistant.
- Collect 2×2 gauze and tape or bandaid
- Wash your hands and don clean gloves
- While holding the catheter in place, start peeling off the Tegaderm and/or tape. Use an alcohol pad if very sticky and painful.
- Once the dressing is no longer secured to the skin, place a 2×2 gauze over the insertion site, and pull out the IV in a smooth fashion.
- Hold pressure for 1-2 minutes until bleeding as stopped
- Dress with gauze and tape or bandaid
WANT TO LEARN MORE?
If you want to learn more about cardiac arrhythmias, I have a complete video course “ECG Rhythm Master”, made specifically for nurses which goes into so much more depth and detail.
With this course you will be able to:
- Identify all cardiac rhythms inside and out
- Understand the pathophysiology of why and how arrhythmias occur
- Learn how to manage arrhythmias like an expert nurse
- Become proficient with emergency procedures like transcutaneous pacing, defibrillation, synchronized shock, and more!
I also include some great free bonuses with the course, including:
- ECG Rhythm Guide eBook (190 pages!)
- Code Cart Med Guide (code cart medication guide)
- Code STEMI (recognizing STEMI on an EKG)
Check out the course!
Checkout Related Content
How to Read an ECG

10 Tips for IV Insertions

STEMI vs NSTEMI

VTACH + VFIB
References
UpToDate & Other Databases
- Intravenous Cannulation (Medscape)
- Peripheral Venous Access in Adults
Textbooks
-
Sheehy’s Manual of Emergency Care, 7th edition (Unit 2, p. 110)
-
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8th edition, (Chapter 31, pp. 198-199)
When do we take off the tourniquet?
0 ReplyDifferent nurses do this differently, but I’d say the best time to take off the tourniquet would be after extracting the needle when your catheter is in place. If you are drawing blood, sometimes leaving the tourniquet on will help you get blood, but will also increase the risk of hemolysis. Definitely make sure to take the tourniquet off before flushing as this could blow the vein.
3 ReplyI once had to have emergency dialysis due to AFR/AFI. Honestly the stent or whatever it was that was put into my femoral vein felt like a garden hose! I am average size. So does anyone else what gauge is used for Emergercy Dialysis?
1 ReplyThat’s Nicely Explain about the IV Cannula.
0 ReplyITS VERY INTERSTING ANS KNOWLEDGE ABLE FOR ALL
0 ReplyLove your content. Very helpful for our new grads. Just an FYI, under contraindications, you have bloot clots instead of blood. 🙂
0 ReplyGlad you like it!! I updated that btw – THANK YOU! 🙂
0 Reply 70Would love your thoughts, please comment.x()x| ReplyInsertTag » How To Start An Iv
-
How To Start An IV: A 5-Step Guide - SimpleNursing
-
How To Start An IV | IV Catheter Insertion & Flush Technique In Hand
-
How To Start An IV - YouTube
-
How To Start An IV | Intravenous Insertion For Nurses - YouTube
-
How To Start An IV? 50+ Tips & Techniques On IV Insertion
-
How To Start An IV | Starting An IV Clinical Nursing Skills
-
4 Secrets Of Smooth IV Starts - Outpatient Surgery Magazine - AORN
-
How Not To Blow Veins When Starting An IV - The IV Guy
-
How To Insert An IV (with Pictures) - WikiHow
-
On The Road To Successful I.V. Starts : Nursing2022 - Lippincott
-
How To Insert An IV : 11 Steps - Instructables
-
Intravenous Cannulation (IV) - Medistudents
-
How To Start An IV | Nursing School Review | NurseMegRN