Pulse & SpO2 - REAL First Aid
Maybe your like
- First Aid Articles
- Overcoming Adrenaline
- Accident Procedure
- Big Sick or Little Sick?
- Pulse & SpO2
- Blood Pressure
- The Art of Questioning - SAMPLE
- The Art of Questioning - PQRST
- Diagnostics
- Ankle Injuries
- Ballistic Injuries
- Blast Injury
- Burns Part 1: Thermal Burns
- Burns Part 2: Special Cases
- Casualty Positioning
- CPR in Remote Environments
- Chest Injury - Closed
- Chest Injury - Open
- Crush Injury
- Drowning
- Eye Injuries
- Extended Field care
- Heat Stroke & Heat Related Illnesses
- Hyponatremia - the effects of over-hydration
- Hypothermia Guidelines
- Lyme Disease
- Managing Musculoskeletal Injuries
- Oxygen - Sometimes Less Is More
- Pain Management
- Pelvic Injury
- Poisoning
- Spinal Injury in Remote Environments
- Suspension Trauma
- Trauma Basics - Catastrophic Haemorrhage
- Trauma Basics - Shock!
- Triage
- Understanding Anaphylaxis
- Understanding Asthma
- Understanding Chest Pain: Part 1 - Heart Attack & Angina
- Understanding Chest Pain: Part 2 - What does Cardiac Arrest Look Like?
- Understanding Chest Pain: Part 3 - Heart Attack & Aortic Aneurysm
- Understanding COPD
- Understanding Diabetes
- Understanding Diarrhoea & Vomiting
- Understanding Epilepsy
- Understanding Menstruation
- Understanding The Hangover
- Understanding Sepsis
- Use of Epi-Pens
Additional Vital Signs: Pulse & SpO2
In addition to the 5 Basic Vital Signs we can add Pulse and Sp02 (Oxygen Saturation), but to do this we require equipment; the Pulse Oximeter.
Pulse
Checking a pulse is hard. On a fit, healthy casualty in low stress situations it can sometimes be easy to feel a nice juicy pulse but in reality, with a poorly casualty, and you’re having a bit of a moment and you are not in a nice, quiet training environment, don’t bother.
In the late 90’s several studies were conducted to assess the accuracy of lay people (1), First Aiders, Paramedics and even Doctors in assessing simply the presence of a pulse. In one study, success rates were as low as 45% in identifying the presence of a pulse (2) and in another, junior doctors took an average of 18 seconds to identify a pulse (3).
It was for these reasons that, based on advice from the International Liaison Committee on Resuscitation, the United Kingdom Resuscitation Council and American Heart Association removed routinely checking for a pulse as a sign of life from First Aid training in the 2000 updates.
But checking a pulse does have value – as with all of the basic vital signs, knowing whether the casualty’s pulse rate is within a normal range can assure us; if the casualty’s pulse is outside of these ranges it can even point us toward a particular problem.
If someone has been running around we would expect their pulse to rise. We’d also expect them to be hot, red and breathing faster.
If they haven’t been running around, but they’re hot, red, fast breathing and with a fast pulse, we may have a problem, this could indicate sepsis.
If they’re a trauma casualty; hot, red and with a slow, strong pulse, this could indicate internal head injury.
If they’re a trauma casualty, cold and pale with a fast pulse, this could be hypovolaemic shock.
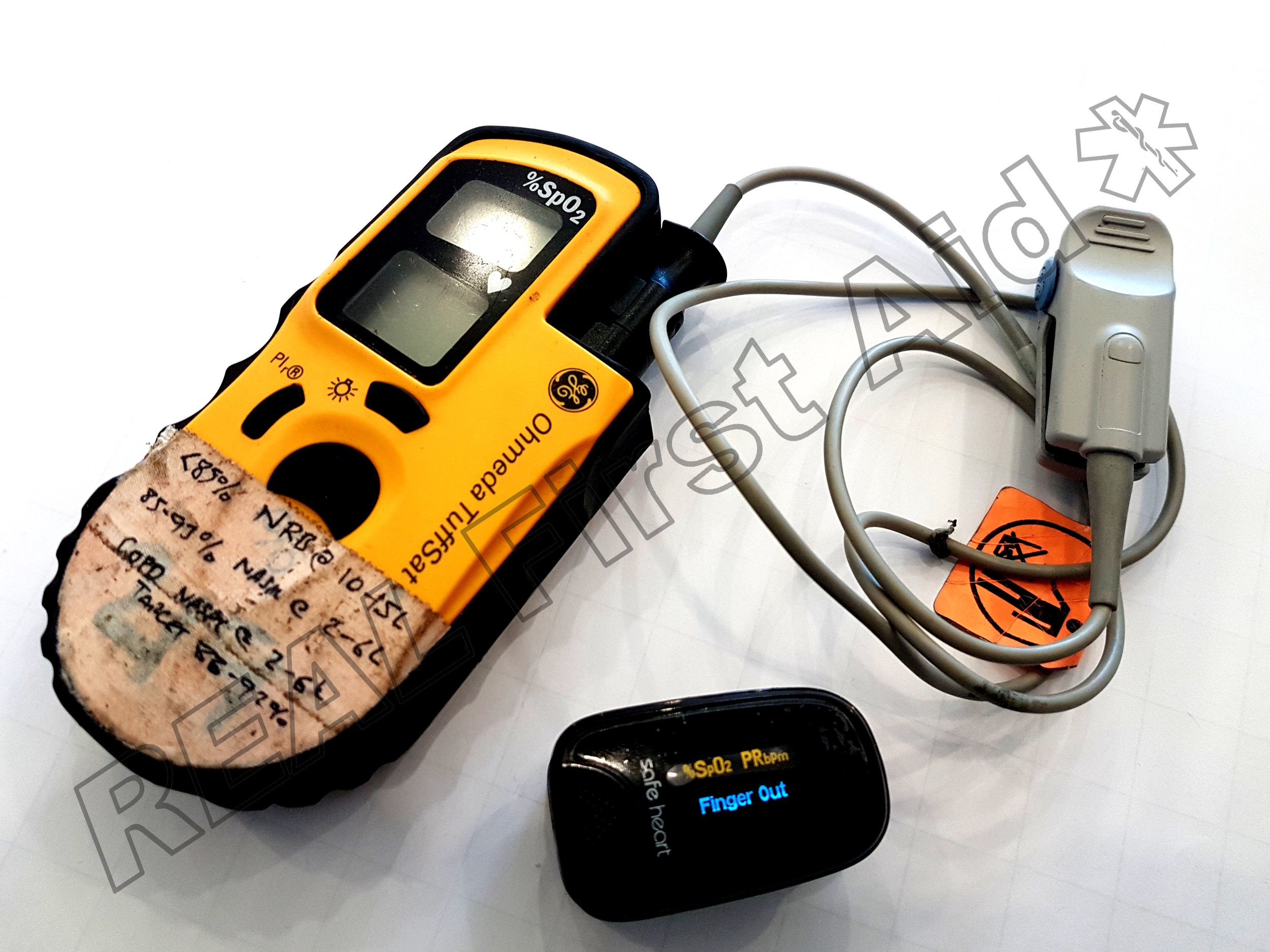
Just don’t bother trying to check it manually. We’re going to use the Pulse Oximiter: The Pulse Oximeter is a small diagnostic tool which is predominantly used to identify the casualty’s oxygen saturations but it will also show the casualty’s pulse. With one of these, we don’t need to be wasting time reaching around the casualty, desperately feeling for a pulse.