B-Cell Lymphoma Workup - Medscape Reference
The histologic findings in B-cell non-Hodgkin lymphoma (NHL) are varied. The salient features of the most common subtypes are described below.
Chronic lymphocytic leukemia/small lymphocytic lymphoma
Chronic lymphocytic leukemia (CLL)/small lymphocytic leukemia (SLL) is a neoplasm composed of monomorphic small, round to slightly irregular B lymphocytes in the peripheral blood, bone marrow, spleen, and lymph nodes, admixed with prolymphocytes and paraimmunoblasts forming proliferation centers in tissue infiltrates.
The lymph node architecture is effaced, with a pseudofollicular pattern of regularly distributed pale areas corresponding to proliferation centers containing larger cells in a dark background of small cells. The predominant cell type is the small lymphocyte. Mitotic activity is usually low. The size of proliferation centers and the number of paraimmunoblasts vary from case to case, but there is no correlation between lymph node histology and clinical course.
On peripheral blood smears and bone marrow aspirate smears the CLL/SLL cells are small lymphocytes with clumped chromatin and scant cytoplasm. Smudge or basket cells are typically seen in peripheral blood smears.
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue
Mucosa-associated lymphoid tissue (MALT) lymphoma is an extranodal lymphoma composed of morphologically heterogeneous small B cells, including marginal zone (centrocytelike) cells, small lymphocytes, and scattered immunoblast and centroblastlike cells.
The lymphoma cells infiltrate around reactive B-cell follicles, external to a preserved follicle mantle, in a marginal zone distribution and spread out to form larger confluent areas that eventually overrun some or most of the follicles. There is plasma cell differentiation in a proportion of the cases. In epithelial tissues, the neoplastic cells typically infiltrate the epithelium, forming lymphoepithelial lesions.
Nodal marginal zone lymphoma
Nodal marginal zone lymphoma (NMZL) is a primary nodal B-cell neoplasm that morphologically resembles lymph nodes involved by marginal zone lymphoma of extranodal or splenic types, but without evidence of extranodal or splenic disease.
Follicular lymphoma
Follicular lymphoma is a neoplasm composed of follicle center B cells (typically both centrocytes and centroblasts) that usually has at least a partially follicular pattern. It is graded by counting or estimating the absolute number of centroblasts in 10 neoplastic follicles, expressed per 40× high-power microscopic field (hpf). Grade 1 and grade 2 cases have a marked predominance of centrocytes and only a few centroblasts (grade 1, 0-5 centroblasts/hpf; grade 2, 6-15 centroblasts/hpf; grade 3, >15 centroblasts/hpf).
 Neoplastic follicles comprising cleaved cells (centrocytes) and larger cells with vesicular nuclei and prominent 2-3 nucleoli (centroblasts). View Media Gallery
Neoplastic follicles comprising cleaved cells (centrocytes) and larger cells with vesicular nuclei and prominent 2-3 nucleoli (centroblasts). View Media Gallery If diffuse areas of any size composed predominantly or entirely of blastic cells are present in any case of follicular lymphoma, a diagnosis of diffuse large B-cell lymphoma (DLBCL) is also made. Peripheral blood involvement sufficient to produce lymphocytosis (usually < 20,000/µL) is observed in about 10% of patients. Bone marrow involvement occurs in 65% of patients and characteristically takes the form of paratrabecular lymphoid aggregates. Splenic white pulp and hepatic portal triads are also frequently involved.
Mantle cell lymphoma
Mantle cell lymphoma is a B-cell neoplasm generally composed of monomorphic small to medium-sized lymphoid cells with irregular nuclear contours and a cyclin-D1 translocation (see the image below). Neoplastic transformed cells resembling centroblasts, immunoblasts, or paraimmunoblasts and proliferation centers are absent. Hyalinized small vessels are commonly seen.
 Mantle cell lymphoma. Small lymphoid cells with oval to slightly irregular nuclei and clumped chromatin and rare admixed pink histiocytes. View Media Gallery
Mantle cell lymphoma. Small lymphoid cells with oval to slightly irregular nuclei and clumped chromatin and rare admixed pink histiocytes. View Media Gallery A spectrum of morphologic variants is recognized. The blastoid and pleomorphic variants are considered to have poorer prognosis and to be of important clinical significance. Further evaluation of the proliferation fraction, either by counting mitotic figures or estimating the proportion of Ki67-positive nuclei, is important because of its prognostic impact.
Diffuse large B-cell lymphoma
The common morphologic features that unite the various forms of DLBCL are the relatively large cell size (usually 4-5 times that of a small lymphocyte) and a diffuse pattern of growth. [17] In other respects, a fair degree of morphologic variation exists.
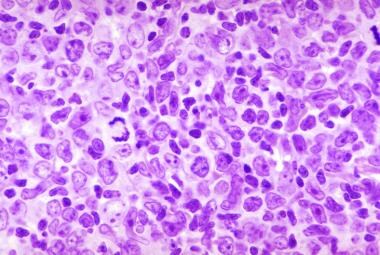
In most cases, the tumor cells have a round or oval nucleus that appears vesicular because of margination of chromatin at the nuclear membrane, but large multilobed or cleaved nuclei predominate in some cases (see the image below). Nucleoli may be 2-3 in number and located adjacent to the nuclear membrane, or they may be single and centrally placed. Cytoplasm is usually present in moderate abundance and may be pale or basophilic.
 Diffuse large B-cell non-Hodgkin lymphoma. Large cells with abundant cytoplasm and large round-ovoid nuclei with thick nuclear membrane and multiple prominent nucleoli. View Media Gallery
Diffuse large B-cell non-Hodgkin lymphoma. Large cells with abundant cytoplasm and large round-ovoid nuclei with thick nuclear membrane and multiple prominent nucleoli. View Media Gallery Other more anaplastic tumors may contain multinucleated cells with large inclusionlike nucleoli that closely resemble Reed-Sternberg cells, and phenotyping is often necessary to distinguish these 2 entities.
An immunophenotypical subdivision of DLBCL has been proposed that uses a combination of antibodies to CD10, bcl-6, and MUM-1 to divide DLBCL into germinal center B cell-like (GCB) and nongerminal center B cell-like (non-GCB) varieties. Cases that are CD10 positive or CD10 negative and bcl-6 positive but MUM-1 negative are regarded as GCB type, whereas all others are regarded as non-GCB or activated B-cell (ABC) type.
This immunophenotypical subdivision does not completely correlate with gene expression-based subgrouping of DLBCL. In the non-GCB or the ABC, bcl-2 expression is known to be associated with poor patient outcome.
DLBCL may be classified in several different ways. Common morphologic variants of DLBCL, not otherwise specified, include centroblastic, immunoblastic, anaplastic, and rare morphologic variants. Molecular subgroups include GCB and ABC. Immunohistochemical subgroups include CD5-positive DLBCL, GCB, and non-GCB.
DLBCL subtypes include the following:
- T-cell/histiocyte rich large B-cell lymphoma
- Primary DLBCL of the central nervous system (CNS)
- Primary cutaneous DLBCL, leg
- Epstein-Barr virus (EBV)–positive DLBCL of the elderly
Other lymphomas of large B cells include the following:
- Primary mediastinal (thymic) large B-cell lymphoma
- Intravascular large B-cell lymphoma
- DLBCL associated with chronic inflammation
- Lymphomatoid granulomatosis
- Anaplastic lymphoma kinase (ALK)-positive large B-cell lymphoma
- Plasmablastic lymphoma
- Large B-cell lymphoma arising in human herpesvirus 8 (HHV-8)–associated multicentric Castleman disease
- Primary effusion lymphoma
Borderline cases include the following:
- B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and Burkitt lymphoma
- B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and classical Hodgkin disease
Burkitt lymphoma
Burkitt lymphoma is a B-cell lymphoma with an extremely short doubling time that often presents in extranodal sites or as an acute leukemia. Involved tissues are effaced by a diffuse infiltrate of monomorphic, medium-sized (nuclei similar or smaller to those of histiocytes) transformed lymphoid cells.
The nuclei are round with finely clumped and dispersed chromatin, with multiple basophilic medium-sized paracentrically situated nucleoli. The cytoplasm is deeply basophilic and usually contains lipid vacuoles (see the images below). A high mitotic index is typical, as is apoptotic tumor cell death, accounting for the presence of numerous tissue macrophages with their ingested tissue debris. These macrophages are often surrounded by a clear space, creating the characteristic starry sky pattern.
 Burkitt lymphoma. Normal architecture is entirely replaced by lymphoma cells and evenly dispersed macrophages, starry sky (250×). View Media Gallery
Burkitt lymphoma. Normal architecture is entirely replaced by lymphoma cells and evenly dispersed macrophages, starry sky (250×). View Media Gallery  Burkitt lymphoma cells with round noncleaved nuclei and strongly basophilic cytoplasm (1000×). View Media Gallery
Burkitt lymphoma cells with round noncleaved nuclei and strongly basophilic cytoplasm (1000×). View Media Gallery Primary mediastinal (thymic) large B-cell lymphoma
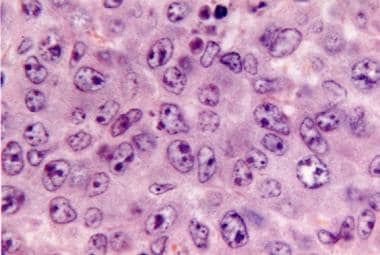
Primary mediastinal large B-cell lymphoma is a diffuse large B-cell lymphoma that arises in the mediastinum from a putative thymic B-cell origin and has distinctive clinical, phenotypic, and genotypic features. Histologically, it is commonly associated with compartmentalizing alveolar fibrosis (see the image below). The cells are medium-sized to large and have abundant clear/pale cytoplasm and round to oval nuclei. A few cases have multilobated and pleomorphic nuclei resembling the Reed-Sternberg cells of Hodgkin lymphoma.
 Compartmentalizing fibrosis and infiltrate of medium-sized to large lymphoid cells. View Media Gallery
Compartmentalizing fibrosis and infiltrate of medium-sized to large lymphoid cells. View Media Gallery Từ khóa » B-nhl Cll
-
NHL Subtypes | Leukemia And Lymphoma Society
-
Types Of B-cell Lymphoma - American Cancer Society
-
Lymphoma - Non-Hodgkin: Subtypes - Cancer.Net
-
Low Grade NHL | Non-Hodgkin Lymphoma - Cancer Research UK
-
Types And Grades | Non-Hodgkin Lymphoma - Cancer Research UK
-
Non-Hodgkin's Lymphoma And Chronic Lymphocytic Leukemia
-
Chronic Lymphocytic Leukaemia (CLL) And Small ... - Lymphoma Action
-
Small B Cell NHL And Their Leukemic Counterpart - PubMed
-
Increasing Incidence Of B-Cell Non-Hodgkin Lymphoma And ... - NCBI
-
Small Lymphocytic Lymphoma - The Leukaemia Foundation
-
NHL & CLL Treatment Option | RIABNI™ (rituximab-arrx)
-
What Are The Types Of B-Cell Lymphoma? - WebMD
-
B-Cell Lymphoma: Practice Essentials, Background, Classification
-
Types Of Non-Hodgkin Lymphoma: Common, Rare And More | CTCA
-
Investigating CD20 CAR T-Cell Therapy In R/R CLL And Other B ...
-
Chronic Lymphocytic Leukemia - Lymphoma Research Foundation
-
Non-Hodgkin Lymphoma: Types, Causes, Symptoms & Treatment