Relevance Of Dynamic Studies With Magnetic Resonance ... - Elsevier
Có thể bạn quan tâm
- Inicio
- Todos los contenidos
- Ahead of print
- Último número
- Todos los números
- Suplementos
- Congresos
- Gastroenterología y Hepatología (English Edition)
- Suscríbase a la newsletter
- Publique su artículo
- Guía para autores
- Envío de manuscritos
- Ética editorial
- Inclusión y diversidad
- Opción Open Access
- Servicios de edición
- Acerca de la revista
- Alcance y objetivos
- Comité editorial
- Suscríbase
- Contactar
- Métricas
- Lo más leído
- Lo más citado
- Más populares
- Todas las métricas
- Métricas por países
 ISSN: 0210-5705
ISSN: 0210-5705 La misión de Gastroenterología y Hepatología es dar cobertura a una amplia gama de temas relacionados con la gastroenterología y hepatología, incluidos los avances más recientes en la patología del tubo digestivo, enfermedad inflamatoria intestinal, hígado, páncreas y vías biliares, siendo una herramienta indispensable para gastroenterólogos, hepatólogos, cirujanos, internistas y médicos generalistas, ofreciendo revisiones exhaustivas y actualizaciones de temas relacionados con la especialidad.
Además de los manuscritos con revisión científica externa sistemática, rigurosamente seleccionados, que se publican en las secciones de investigación (artículos de investigación, cartas científicas, editoriales y cartas al director), la revista también publica guías clínicas y documentos de consenso de las principales sociedades científicas. Es la revista oficial de la Asociación Española de Gastroenterología (AEG), de la Asociación Española para el Estudio del Hígado (AEEH), del Grupo Español de Trabajo en Enfermedad de Crohn y Colitis Ulcerosa (GETECCU) y de la Sociedad Española de Enfermedad Celíaca (CEEC). La publicación está incluida en Medline/Pubmed, en el Science Citation Index Expanded, y en SCOPUS.
Ver más Opción Open AccessIndexada en:
Scopus, Medline, Science Citation Index Expanded (SCIE), SCImago Journal Rank (SJR), SNIP
Ver másSíguenos:
Twitter RSS Alerta emailSuscribirse:
 Factor de impacto
Factor de impacto El factor de impacto mide la media del número de citaciones recibidas en un año por trabajos publicados en la publicación durante los dos años anteriores. © Clarivate Analytics, Journal Citation Reports 2025
Ver más Factor de impacto 2024 1,9 CitescoreCiteScore mide la media de citaciones recibidas por artículo publicado.
Ver más Citescore 2024 1,8 SJRSJR es una prestigiosa métrica basada en la idea de que todas las citaciones no son iguales. SJR usa un algoritmo similar al page rank de Google; es una medida cuantitativa y cualitativa al impacto de una publicación.
Ver más SJR 2024 0,373 SNIPSNIP permite comparar el impacto de revistas de diferentes campos temáticos, corrigiendo las diferencias en la probabilidad de ser citado que existe entre revistas de distintas materias.
Ver más SNIP 2024 0,357 Ver más métricas Ocultar Información de la revista Artículo anterior | Artículo siguiente Vol. 43. Núm. 4.Páginas 179-187 (Abril 2020) Exportar referencia Compartir Compartir Twitter Facebook Linkedin whatsapp E-mail Imprimir Descargar PDF Más opciones de artículo Estadísticas Apartados- Abstract
- Keywords
- Resumen
- Palabras clave
- Introduction
- Abstract
- Keywords
- Resumen
- Palabras clave
- Introduction
- Materials and methods
- Entero magnetic resonance imaging
- Surgery
- Pathology report
- Statistical analysis
- Results
- Discussion
- Conflict of interest
- Bibliografía

 Tablas (6)Table 1. Protocol for magnetic resonance enterography image acquisition.
Tablas (6)Table 1. Protocol for magnetic resonance enterography image acquisition.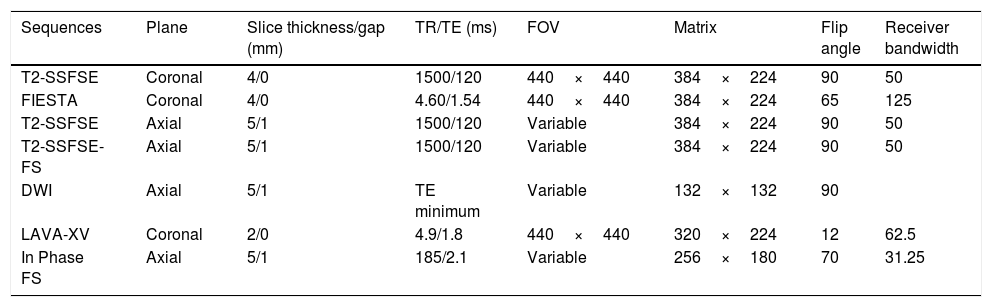 Table 2. Histological Chiorean classification modified by the authors.
Table 2. Histological Chiorean classification modified by the authors. Table 3. Demographic and clinical data of patients (N=28). Age at diagnosis, disease location and behavior were defined according to the Montreal classification.19,20
Table 3. Demographic and clinical data of patients (N=28). Age at diagnosis, disease location and behavior were defined according to the Montreal classification.19,20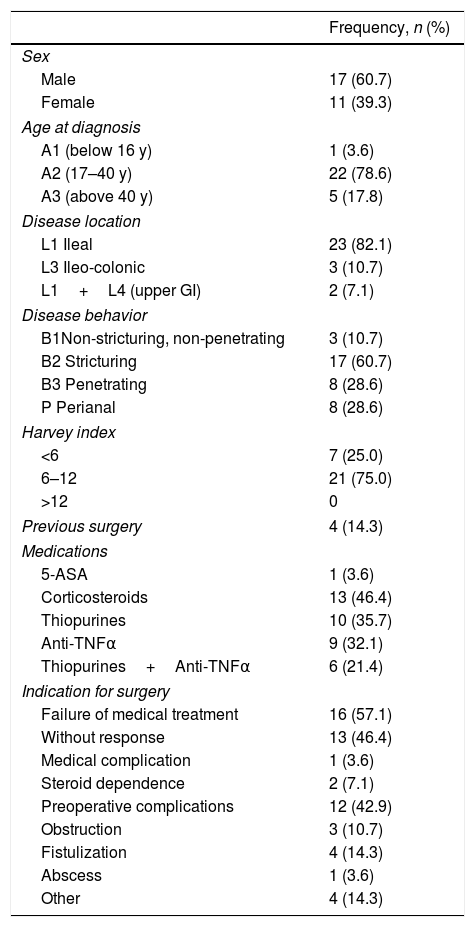 Table 4. Results of correlation between dynamic curve pattern with histological study.
Table 4. Results of correlation between dynamic curve pattern with histological study.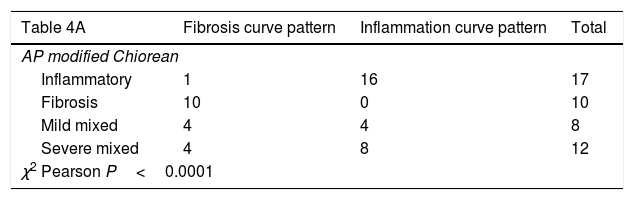 Table 5. Correlation between dynamic curve pattern with the inflammation degree in the histological study.
Table 5. Correlation between dynamic curve pattern with the inflammation degree in the histological study.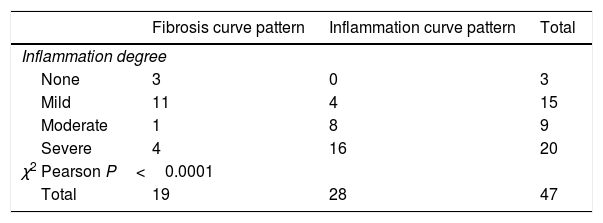 Table 6. Correlation between the dynamic curve pattern with the fibrosis degree in the histological study.
Table 6. Correlation between the dynamic curve pattern with the fibrosis degree in the histological study.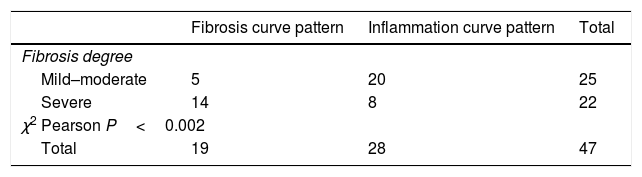 Mostrar másMostrar menos AbstractIntroduction
Mostrar másMostrar menos AbstractIntroductionA proper quantification of the inflammatory activity in Crohn's disease (CD) lesions is needed to establish the appropriate management for each patient. The aim of this study is to evaluate the inflammatory activity of affected segments in small bowel lesions using dynamic studies of magnetic resonance enterography (MRE) in patients undergoing surgery, and their correlation with the level of inflammation and histological fibrosis of the surgical piece.
MethodsA prospective, consecutive, observational, clinical study was conducted that included all the patients with small bowel CD that underwent surgery in this center between March 2011 and September 2013. Diagnosis was established according to Lennard–Jones criteria and the Montreal classification. All the patients underwent MRE within three months before surgery, using a routine protocol involving Liver Acquisition with Volume Acceleration-Extended Volume (LAVA-XV) sequence for the dynamic studies before intravenous administering of gadolinium and 30, 70, 120, and 420s after administering this. The results allowed the designing of graphics with different uptake patterns. The Chiorean classification was used in the histological analysis, as well as a modified version published previously by this study group.
ResultsA total of 28 patients with 47 lesions were analyzed. There was a significant correlation between both curve patterns, including the modified Chiorean classification (P<0.0001) as well as the level of inflammation (P<0.0001) and fibrosis (P<0.002). Inflammatory patterns of dynamic studies are related to histological findings with 80.9% accuracy (sensitivity=75.7%; specificity=100%).
ConclusionThere is a high correlation between dynamic enhancement studies and the level of inflammatory activity. MRE is a suitable tool to differentiate between inflammatory and fibrotic lesions, making it useful to decide the appropriate management of each patient.
Keywords:MRI enterographyCalprotectinSurgeryCrohn's diseaseActivityDiagnosisResumenIntroducciónSe necesita una cuantificación adecuada de la actividad inflamatoria en las lesiones de la enfermedad de Crohn (EC) para establecer el tratamiento adecuado para cada paciente. El objetivo de este estudio es evaluar la actividad inflamatoria de los segmentos afectados en las lesiones del intestino delgado mediante estudios dinámicos de enterografía por resonancia magnética (ERM).
MétodosEstudio prospectivo, consecutivo, observacional y clínico, que incluye a todos los pacientes con EC del intestino delgado que se sometieron a cirugía en nuestro centro entre marzo de 2011 y septiembre de 2013. El diagnóstico se estableció de acuerdo con los criterios de Lennard-Jones y la clasificación de Montreal. Todos los pacientes se sometieron a una ERM dentro de los 3 meses previos a la cirugía, aplicando el protocolo de rutina y secuencias preestablecidas. Para el estudio dinámico se empleó la secuencia Adquisición hepática con aceleración de volumen-Volumen extendido (LAVA-XV), antes de la administración intravenosa (iv) de gadolinio, y 30, 70, 120 y 420s después de esta administración. Los resultados permiten diseñar gráficos con diferentes patrones de captación. En el análisis histológico se utilizó la clasificación de Chiorean, así como una versión modificada creada por nuestro grupo de estudio.
ResultadosEn total se analizaron 28 pacientes con 47 lesiones. Se detectó una correlación significativa entre ambos patrones de curva, incluyendo la clasificación de Chiorean modificada (p<0,0001), así como el grado inflamatorio (p<0,0001) y de fibrosis (p<0,002). Los patrones inflamatorios de los estudios dinámicos se relacionaron con los hallazgos histológicos con una precisión del 80,9% (S=75,7%; E=100%).
ConclusiónExiste una alta correlación entre los estudios dinámicos y el grado de actividad inflamatoria. La ERM constituye una herramienta adecuada para diferenciar entre lesiones inflamatorias y fibróticas, siendo útil para colaborar en la decisión terapéutica.
Palabras clave:Enterografía de resonancia magnéticaCalprotectinaCirugíaEnfermedad de CrohnActividadDiagnóstico Texto completo IntroductionCrohn's disease (CD) is a chronic inflammatory pathology that affects the entire digestive tract. The inflammation has a transmural character that involves the entire thickness of the intestinal wall. Despite the progress in the medical treatment of CD, there is still an increased risk of a surgical intervention.
Inflammatory activity in CD is classically measured by clinical, endoscopic and radiological indicators, and by biological markers. Dynamic studies of entero-magnetic resonance imaging (MRE) have a high sensitivity for the detection of wall and extramural lesions and constitute a well-accepted tool for diagnosis and follow-up 1in patients with CD. Some studies have attempted to relate MRI radiological findings with the severity and activity of the CD,2–5 and some have been able to validate these radiological findings with the histology of the surgical specimen.6–8 Usually, morphological changes related to CD activity are assessed, such as wall thickness, contrast uptake, stenosis, mucous membrane distortions, ulcers, cobblestone appearance, edema, hyper vascularization, pathological lymph nodes, abscess, fistulas, adipose-fibrous proliferation, layers enhancement, pre-stenosis dilation, etc. Radiological indicators based on these findings have even been described to evaluate CD activity and intensity.3,5,9 Several publications try to correlate dynamic pattern of wall enhancement with the extent of inflammation in CD, although they all present different methodology and results.10–16 In a very recent systematic review that reviews the state of the art to assess stenosis and fibrotic component in Crohn's disease, the authors conclude that more studies are needed to distinguish fibrosis from inflammation since the studies published to date are not accurate enough to be used in daily clinical practice.17
It would be interesting to know whether dynamic uptake MRI studies allow differentiating early inflammatory processes of CD, which are susceptible to pharmacological treatment, from fibrotic lesions, with low response to medication, which will probably benefit from surgical treatment.
The aim of this study is to assess the inflammatory activity of CD affected areas in small bowel lesions through dynamic studies of entero-magnetic resonance imaging (MRE) in patients undergoing surgery and to explore their correlation with the degree of inflammation and histological fibrosis of the surgical piece.
Materials and methodsThis is a consecutive, prospective, observational clinical 30-month study (March, 2011–September, 2013), carried out at a tertiary hospital. The study protocol was approved by the Hospital Ethics Committee. All the patients accepted to participate in the study by signing an informed consent form. During the study period, all the patients diagnosed with CD, who were older than 14 years old, presented small bowel affection, and needed surgery due to medical treatment failure or complications, were studied by entero-MRI (n=38). A dynamic study was performed in 28 of these patients, and they were therefore considered for this analysis.
CD diagnosis was defined according to the ECCO standard criteria18 and after excluding infectious, ischemic or vascular, malignant and actinic causes. Patients were classified by age at the moment of diagnosis, location and the disease's behavior. Harvey and Bradshaw Index was used to describe the clinical activity of the CD.19 A preoperative colonoscopy was performed in all the patients, to discard colic affection and, when possible, take a biopsy of the terminal ileum. A multidisciplinary committee discussed each case and made all the decisions related to the management of these patients.
Entero magnetic resonance imagingEvery patient underwent an MRE test during the three months prior to surgery (one month if the patient had received treatment with anti-TNF biological drugs). MRE examinations were performed using a standardized clinical protocol on a 3T magnet (GE MedicalSystems, Milwaukee, WI, USA). Patients fasted for at least 6h and then ingested 1500ml of a 5% mannitol solution over 45min immediately before MRI took place, to distend the small bowel. To reduce bowel peristalsis, 10mg of e.v. hyoscine butylbromide (Buscopan; Boehringer Ingelheim, Ingelheim, Germany) were administered prior to initiating the study, and additional 10mg were administered before administrating the contrast bolus. In case of contraindication (glaucoma, arrhythmia, benign prostatic hypertrophy), 1mg of e.v. glucagon (Glucagen; Novo Nordisk, Bagsvaerd, Denmark) was administered. For the dynamic study, a contrast injection of gadobenate dimeglumine (Multihance; Bracco Diagnostics Inc., Milan, Italy): 0.2ml/kg body weight was administered at a rate of 2ml/s. Images were obtained by placing the patient in prone position. Sequences and parameters of the MRE protocol are detailed in Table 1. Every lesion was listed and measured on a map, starting from the closest to the ileocecal valve. The distance of each lesion from the ileocecal valve, its length and morphological characteristics were precisely measured.
Table 1.Protocol for magnetic resonance enterography image acquisition.
| Sequences | Plane | Slice thickness/gap (mm) | TR/TE (ms) | FOV | Matrix | Flip angle | Receiver bandwidth |
|---|---|---|---|---|---|---|---|
| T2-SSFSE | Coronal | 4/0 | 1500/120 | 440×440 | 384×224 | 90 | 50 |
| FIESTA | Coronal | 4/0 | 4.60/1.54 | 440×440 | 384×224 | 65 | 125 |
| T2-SSFSE | Axial | 5/1 | 1500/120 | Variable | 384×224 | 90 | 50 |
| T2-SSFSE-FS | Axial | 5/1 | 1500/120 | Variable | 384×224 | 90 | 50 |
| DWI | Axial | 5/1 | TE minimum | Variable | 132×132 | 90 | |
| LAVA-XV | Coronal | 2/0 | 4.9/1.8 | 440×440 | 320×224 | 12 | 62.5 |
| In Phase FS | Axial | 5/1 | 185/2.1 | Variable | 256×180 | 70 | 31.25 |
SSFSE, single-shot fast spin echo; FIESTA, fast imaging employing steady state acquisition; FS, fat saturation; DWI, diffusion-weight imaging; LAVA-XV, Liver Acquisition with Volume Acceleration-Extended Volume.
For the dynamic study, Liver Acquisition with Volume Acceleration-Extended Volume (LAVA-XV) sequences prior to contrast administration were used, and also 30, 70, 120 and 420s after the gadolinium administration. In this study, the area of radiological interest (ARI) was placed in the wall section with maximum initial contrast uptake. Enhancement curves were obtained using FuncTool® in the Windows platform version4.8 (GE Medical Systems, Milwaukee, WI, USA) for the analysis of the dynamic pattern of wall enhancement.
The curves were classified as inflammatory pattern when a steep ascending slope in the early phases of contrast uptake in the dynamic study (above 200%), and a decreasing grade of enhancement at the end of the curve was presented. A fibrosis type pattern was determined when the curve displayed a slowly rising slope during the early phases (always below 200%), reaching a plateau or keeping a progressive increase until the end of the curve with no decrease at the end. The decrease in the parietal enhancement degree at the end of the uptake curve was considered distinctive of the inflammatory pattern (Fig. 1). All the images were evaluated by two radiologists experienced in abdominal imaging who reached a consensus regarding any doubts about the interpretation of the images. Both radiologists were blinded to the clinical and laboratory data.
 Figure 1.
Figure 1. Magnetic resonance enterography and pattern curves. Image A represents inflamed bowel area and its corresponding inflammatory enhancement curve. Image B represents a fibrotic stenosis and its corresponding enhancement curve.
SurgeryAll the patients were operated on by members of the Colorectal Surgery Unit, under homogenous surgical criteria and applying the same perioperative protocol. Elective laparoscopic ileocaecal or ileocolonic resection with latero-lateral anastomoses was the most common procedure (n=20 patients). All the resected bowel segments were remitted for pathological examination, indicating whether one or more lesions were included, its number and location, specifying its distance from the ileocecal valve. When necessary, a picture describing the location of the resected segments was sent along with the specimens. When a strictureplasty was performed, complete wall samples were obtained for histological study.
Pathology reportThe freshly excised specimen was photographed before fixation in 10% formaldehyde solution during 24h. Fibrosis and inflammation of the lesions were defined according to the Chiorean criteria.20 A lesion presenting moderate or severe inflammation and none, mild or moderate fibrosis was defined as “Inflammatory”. A lesion displaying severe fibrotic component and none or mild inflammation was defined as “Fibrotic”. In all the other cases lesions were defined as “Mixed”. In this manuscript, a modification of the Chiorean Classification was used dividing the mixed group in mild mixed (no or mild inflammation and mild or moderate fibrosis) and severe mixed (moderate or severe inflammation and severe fibrosis) (Table 2). Two experienced Pathologists, specialized in digestive diseases and part of the multidisciplinary team, evaluated all the specimens. In case of discrepancies, data interpretation was made by consensus.
Table 2.Histological Chiorean classification modified by the authors.
| Inflammation score (0=none; 1=mild; 2=moderate; 3=severe) | Fibrosis score (0=none; 1=mild or moderate; 2=severe) | Lesion with predominant component: |
|---|---|---|
| >1 | ≤1 | Inflammatory |
| ≤1 | >1 | Fibrotic |
| Difference ≤1 | Mixed | |
| 1 or 0 | 1 | Mild mixed |
| 3 or 2 | 2 | Severe mixed |
Data was analyzed by patients and by lesions. Lesion analysis was accomplished by correlating pathologically assessed surgical specimen's lesions, with the ones identified on the MRE. Unconfirmed lesions during surgery, have been excluded from the analysis.
The Variable Statistics were attained by using the IBM® SPSS® Statistical Program for Social Science version 22.0. In the univariate analysis, continuous variables were expressed using the mean and the standard deviation, while categorical variables were expressed using frequencies and percentages (number of patients, number of lesions, and the percentage). When a non-parametric analysis of categorical variables was necessary, the Pearson's Chi-square test was applied. For the analysis of dichotomous MRI results, a 2×2 table was used and, values of sensitivity, specificity, diagnostic accuracy, positive predictive value (PPV) and negative predictive value (NPV) were obtained by calculating 95% confidence intervals for all estimates. P value of
Từ khóa » Dynamic Mri Là Gì
-
Chụp Cộng Hưởng Từ Tuyến Yên Có Tiêm Thuốc đối Quang Từ (khảo Sát ...
-
Chụp Cộng Hưởng Từ (MRI) Tiền Liệt Tuyến | Vinmec
-
Chụp Cản Từ động Trong đánh Giá Ung Thư Dynamic Contrast ...
-
Chụp Cộng Hưởng Từ Tuyến Yên Có Tiêm Thuốc đối Quang ...
-
Vai Trò Chụp Cộng Hưởng Từ MRI Tuyến Tiền Liệt
-
Tổng Quan Về Kỹ Thuật Cộng Hưởng Từ Tuyến Tiền Liệt đa Thông Số ...
-
Chụp Cộng Hưởng Từ Tuyến Yên Có Tiêm Thuốc đối Quang Từ (khảo Sát ...
-
VAI TRÒ CỦA CỘNG HƯỞNG TỪ ĐỘNG TRONG CHẨN ĐOÁN ...
-
[PDF] CHẨN ĐOÁN HÌNH ẢNH U TUYẾN YÊN - VNU
-
Những Chỉ định Cộng Hưởng Từ (MRI) Tuyến Vú Hiện Nay
-
Dynamic MRI For Articulating Joint Evaluation On 1.5 T And 3.0 ... - NCBI
-
Dynamic MRI Of The Wrist In Less Than 20 Seconds - NCBI
-
[PDF] NGHIÊN CỨU ĐẶC ĐIỂM HÌNH ẢNH VÀ VAI TRÒ CỘNG HƯỞNG ...