The Obstetric History - OSCE - Gravidity - Parity - TeachMeObGyn
- History Taking and Examinations
- History Taking
- The Obstetric History
Written by Minesh Mistry
Last updated 4th December 2024 • 10 Revisions •
Contents- Previous Obstetric History
- Current Pregnancy
- Past Medical History
- Drug History
- Family History
- Social History
The Obstetric History - Podcast Version
TeachMeObGyn
0:00 / 0:00 1x- 0.25x
- 0.5x
- 0.75x
- 1x
- 1.25x
- 1.5x
- 1.75x
- 2x
Pregnancy can be a time of great excitement to the patient, but it can also be a time of danger, and there are certain serious illnesses of pregnancy to be aware of.
Below, we will provide a framework for capturing a basic obstetric history.
Note: In the UK, pregnant women attend a booking appointment with a midwife at between 8 and 12 weeks’ gestation. Much of the history is covered here and documented in notes that the patient is advised to carry at all times. An example can be viewed on the Perinatal Institute website.
Previous Obstetric History
A good starting point is to ask about number of children the patient has given birth to. Next, sensitively ask about miscarriages, stillbirths, ectopics and terminations.
Term Pregnancies
For each previous pregnancy carried beyond 24 weeks, inquire about the following:
- Gestation – previous preterm labour is a risk factor for subsequent preterm labour.
- Mode of delivery – spontaneous vaginal, assisted vaginal or Caesarean.
- Gender
- Birth weight – a previous small for gestational age (SGA) baby increases the risk of a subsequent one.
- Complications – e.g. pre-eclampsia, gestational hypertension, gestational diabetes, obstetric anal sphincter injury (3rd, 4th degree tears), post-partum haemorrhage.
- Assisted reproductive therapies (ART) – e.g. ovulation induction with clomiphene, IVF.
- Care providers – was the patient’s care completely with a midwife or was there previous obstetric input, if so, why
ART pregnancies are often conceived after a long period of time and after much psychological distress; it is important to be aware of this. In addition, use of ARTs can increase the risk of pre-eclampsia during pregnancy.
Other Pregnancies
For pregnancies not carried beyond 24 weeks, inquire about:
- Gestation – miscarriages can be classified into early pregnancy (12 weeks or less) or second trimester (13-24 weeks).
- Miscarriages – outcome (spontaneous, medical management, surgical management – evacuation of retained products of conception).
- Terminations – method of management: medical or surgical.
- Identified causes of miscarriage / stillbirth – e.g. abnormal parental karyotype, fetal anomaly.
For ectopic pregnancies, ask about:
- Site of the ectopic
- Management: expectant (monitoring of serum hCG levels), medical (methotrexate injection), surgical (laparoscopy or laparotomy; salpingectomy (removal of tube) or -otomy (cutting of tube and suctioning of trophoblastic tissue))
Gravidity and Parity
Gravidity is the total number of pregnancies, regardless of outcome. Parity is the total number of pregnancies carried over the threshold of viability (24+0 in the UK).
Examples [Macleod’s 2005, p.212]:
- Patient is currently pregnant; had two previous deliveries = G3 P2
- Patient is not pregnant, had one previous delivery = G1 P1
- Patient is currently pregnant, had one previous delivery and one previous miscarriage = G3 P1+1 (the +1 refers to a pregnancy not carried to 24+0).
- Patient is not currently pregnant, had a live birth and a stillbirth (death of fetus after 24+0) = G2 P2
- Patient is not pregnant, had a twin pregnancy resulting in two live births = G1 P1
Current Pregnancy
First, ask about the gestational age of the pregnancy. Gestation is described as weeks+days (e.g. 8+4; 30+7; 40+12 – post-dates).
The last menstrual period date (LMP) can be used to estimate gestation, with Naegele’s rule the most common method (to the first day of the LMP add 1 year, subtract 3 months, add 7 days). This can be imprecise, as it requires accurate recall of LMP dates as well as regular menstruation.
Instead, pregnancies are dated based on the crown-rump length (CRL), measured by ultrasound scan between 10+0 and 13+6. This way, we avoid unnecessary inductions for ‘post-dates’ based on LMP recalled later than in reality, and we can monitor labours where the LMP date suggests is over 37+0 but the scan suggests is preterm.
In the history of current pregnancy, ask about:
- Has there been use of folate prior to conception and currently
- Agreed estimated date of delivery (EDD): this date is when the woman will be 40+0.
- Singleton or multiple gestation.
- Uptake and results of Down’s syndrome screening (if scanned between 11+0 and 13+6).
At 18+0 to 20+6, women are offered a scan to check for fetal anomalies. Be sure to review the findings of this scan:
- Fetal anomalies – presence or absence.
- Placenta position – check it is clear of the internal os.
- Amniotic fluid index – oligohydroaminos, normal or polyhydraminos
- Estimated fetal weight – parameter for growth

Fig 1Ultrasound scan of a pregnancy at 12 weeks, showing the measurement of the crown-rump length.
Past Medical History
Ask the usual questions about past medical history, abdominal or pelvic surgery and mental health conditions. Remember that the medical co-morbidities that are most likely to affect women of childbearing age include:
- Asthma
- Cystic fibrosis
- Epilepsy
- Hypertension (older women)
- Congenital heart disease
- Diabetes – check if type 1 or type 2
- Systemic autoimmune disease e.g. systemic lupus erythematosus (SLE), rheumatoid arthritis
- Haemoglobinopathies: sickle-cell disease, thalassaemias
- Blood-borne viruses: HIV, hepatitis B, hepatitis C
Mental Health
Mental health is extremely important – in the Saving Mothers’ Lives report covering 2011-2013 [MBRRACE-UK 2015], it was identified that nearly 25% of deaths occurring six months to a year post-partum were due to psychiatric causes. The same report advised the following as ‘red flags’ to arranging urgent senior psychiatric assessment:
- Recent significant change in mental state or emergence of new symptoms
- New thoughts or acts of violent self-harm
- New and persistent expressions of incompetency as a mother, or of estrangement from the infant
Inquire about previous psychiatric disorder, to include depression, anxiety disorders, bipolar affective disorder, schizophrenia, previous self-harm or suicide attempts.
Drug History
In addition to asking about drug allergies and intolerances, be aware that the embryonic (first 12 weeks) period of pregnancy is thought to be the time of most sensitivity for drugs to cause fetal structural defects (teratogenicity). Thus, inquire about drugs taken around conception and during the first 12 weeks.
Inquire about drugs currently being taken (include herbal/complementary therapies). Ask about illicit drugs and alcohol – recommend the patient to stop these drugs, and to offer referral to help-to-quit services too.
Recommend that the patient takes 400μg folic acid per day for the first 12 weeks, to reduce the chance of the baby developing a neural tube defect. [NICE CG62, 2016] – 1.3.2.1.
Family History
Although not usually regarded as a substantial part of the obstetric history, there is increasing evidence that certain conditions are associated with adverse pregnancy outcomes.
Conditions such as cystic fibrosis and sickle-cell disease are heritable – the patient should be counselled as to the risk of her baby developing these conditions (based on the parental genotypes).
A family history of type 2 diabetes in a first degree relative is considered a risk factor for developing gestational diabetes.
By Cburnett [CC-BY-SA-3.0], via Wikimedia Commons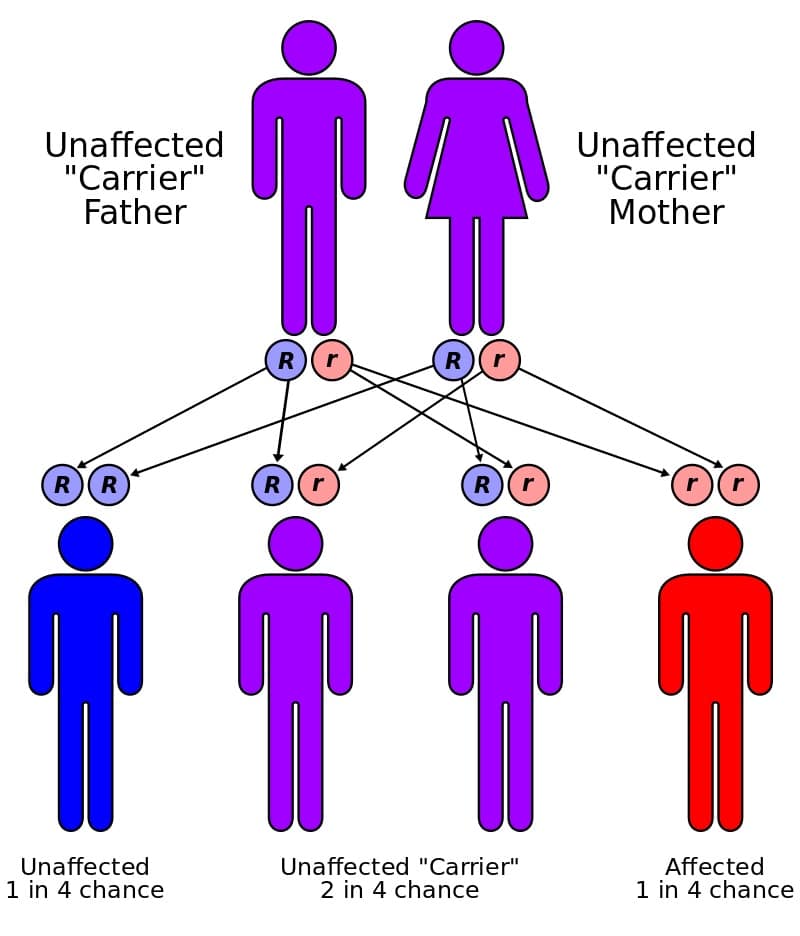
Fig 2Mode of inheritance of autosomal recessive conditions, such as cystic fibrosis.
Social History
Pregnancy can be a time of great elation, intense anxiety – and quite possible a mixture of anything and everything between. Ask the patient about her thoughts of the pregnancy; be sensitive if the pregnancy is unplanned.
Ask about current / previous occupation, and plans for returning to work (or otherwise).
Inquire about home circumstances: e.g. who does the patient live with – partner / spouse? Children in the home? Ask also about support networks, e.g. parents / in-laws, neighbours, friends.
Inquire about financial circumstances – the cost of caring for a child in addition to being out of work can potentially have an adverse impact on the patient’s ability to cope financially. Is the patient eligible for social security / child benefit payments?
Ask about smoking – how many per day; what drug (tobacco, cannabis, others); duration of smoking. Would the patient like to quit, and would they like help with this? Reiterate the association between smoking and small-for-gestational-age babies [RCOG GTG31, 2014], and offer her help to quit.
It is also important to remember that at least once during the course of the pregnancy, women should be asked whether they are victim to domestic abuse.
Rate This ArticleRecommended Reading
Login
Log in with Google Username or Email Password Forgotten Password Back to Sign Up Sign In No account yet? Register nowForgot Password
Please enter your username or email address below. You will receive a link to create a new password via emai and please check that the email hasn't been delivered into your spam folder.
Username or Email Back to Login Reset Password This website uses cookies.We use cookies to improve your experience on our site and to show you relevant advertising. To find out more, read our privacy policy.
Accept ClosePrivacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience. Necessary Necessary Always Enabled Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |
Help Us Improve This Question
SubmitRate This Article
SubmitTừ khóa » G2 P1 C1 A0
-
Gravida & Parity: Definition & Examples - Video & Lesson Transcript
-
Gravidity And Parity Definitions (Implications In Risk Assessment)
-
What Is It G2P1 In Medical Field? - WordReference Forums
-
Gravidity And Parity - Wikipedia
-
On The Efficiency Of Competitive Stock Markets Where Trades ... - Jstor
-
NYC Building Classifications - DOF
-
[PDF] ENGN1630-20-fast-adder.pdf
-
SOLUTIONS
-
Low Birth Weight In Pregnancies Following Induced Abortion - PubMed
-
Obstetrics Words | Gravida Para Abortus - Meditec
-
[PDF] Combinational Logic Design Case Studies Arithmetic Circuits
-
[PDF] CIS 371 Computer Organization And Design
-
[PDF] ECE 380: Control Systems - Purdue Engineering