Graves Disease With Negative TSH Receptor Antibodies
- Home
- All contents
- Ahead of print
- Latest issue
- All issues
- Special issues & Supl.
- Subscribe to our newsletter
- Publish your article
- Guide for authors
- Submit an article
- Ethics in publishing
- Diversity pledge
- Language Editing services
- Conflict of interest
- About the journal
- Aims and scope
- Editorial Board
- Contact
- Metrics
- Most often read
- All metrics
 ISSN: 2341-2879
ISSN: 2341-2879 The Spanish Pediatric Association (Asociación Española de Pediatría, AEP) has as one of its main objectives the dissemination of rigorous and up-to-date scientific information on the various areas of pediatrics. Annals of Pediatrics is an open access journal that serves as the Association's Scientific Expression Organ and constitutes the vehicle through which members communicate. Annals of Pediatrics publishes, in English and Spanish, original research papers on pediatrics, as well as review articles prepared by experts in each specialty, and guidelines or positioning documents prepared by the different Societies/Specialized Sections integrated into the Spanish Pediatric Association. The journal, a reference for Spanish-speaking pediatrics, is indexed in the most important international databases: Index Medicus/Medline IBECS, IME, SCOPUS, Science Citation Index Expanded, Journal Citations Report, Embase/Excerpta Medica, Directory of Open Access Journals (DOAJ).
See moreIndexed in:
Medline, Directory of Open Access Journals (DOAJ)
See moreFollow us:
RSS Alerta email Impact factorThe Impact Factor measures the average number of citations received in a particular year by papers published in the journal during the two preceding years. © Clarivate Analytics, Journal Citation Reports 2025
See more Impact factor 2024 2.1 CitescoreCiteScore measures average citations received per document published.
See more Citescore 2024 1.9 SJRSRJ is a prestige metric based on the idea that not all citations are the same. SJR uses a similar algorithm as the Google page rank; it provides a quantitative and qualitative measure of the journal's impact.
See more SJR 2024 0.353 SNIPSNIP measures contextual citation impact by wighting citations based on the total number of citations in a subject field.
See more SNIP 2024 0.602 View more metrics Hide Journal Information Previous article | Next article Vol. 93. Issue 6.Pages 417-419 (1 December 2020) Lee este artículo en Español Export reference Share Share Twitter Facebook Linkedin whatsapp E-mail Print Download PDF More article options Statistics Vol. 93. Issue 6.Pages 417-419 (1 December 2020) Scientific letter DOI: 10.1016/j.anpede.2020.01.014 Open Access Graves disease with negative TSH receptor antibodies: a presentation of 5 cases Enfermedad de Graves con autoanticuerpos contra el receptor de la TSH negativos: a propósito de 5 casos Visits 33621 Download PDF Aina Scatti Regàsa, Corresponding author [email protected]Corresponding author. , Ricard Pujol Borrellb, Roser Ferrer Costac, Elsa Puerto Carranzad, María Clemente Leónea Servicio de Pediatría, Hospital Universitario Vall d’Hebron, Barcelona, Spainb Servicio de Inmunología, Hospital Universitario Vall d'Hebron, Barcelona, Spainc Servei de Bioquímica Clínica, Hospital Universitario Vall d’Hebron, Barcelona, Spaind Unidad de Endocrinología Infantil, Institut d’Investigació Biomèdica de Girona Doctor Josep Trueta (IDIBGI), Girona, Spaine Unidad de Endocrinología Pediátrica, Hospital Vall d´Hebron, Grupo de Investigación Crecimiento y Desarrollo, Instituto Investigación Vall d´Hebron (VHIR), CIBER de Enfermedades Raras, Instituto Salud Carlos III, Universitat Autònoma de Barcelona, Barcelona, Spain This item has received 33621 Visits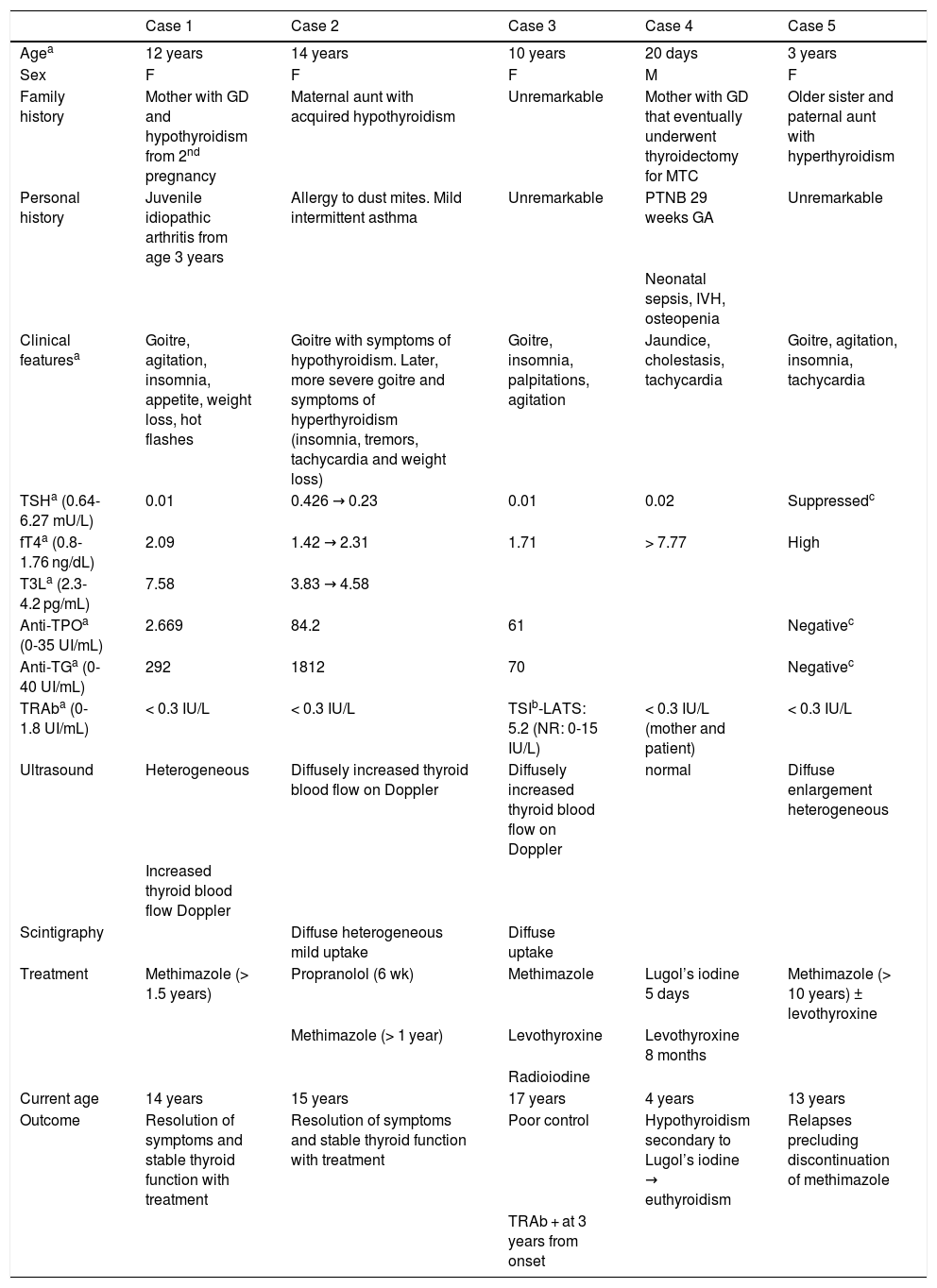 Full Text To the Editor:
Full Text To the Editor: Graves disease (GD) is the leading cause of hyperthyroidism in the paediatric population. It is an autoimmune disease characterised by the production of antibodies against the thyroid stimulating hormone receptor (TSHR) and progressive infiltration of the thyroid by T and B lymphocytes.1
There are 3 types of antibodies that bind TSHR, or thyroid receptor antibodies (TRAb): thyroid-stimulating antibodies (TSAb); TSH-stimulation blocking antibodies (TBAb) and so-called “neutral” TRAb.1 These antibodies can be detected by immunoassays with a sensitivity of up to 98% in third-generation binding assays,1,2 or by means of cell-based bioassays, which measure functional activity and may even be more sensitive.1–3
The diagnosis of GD is based on the detection of lower-than-normal levels of TSH and presence of TRAb.4 However, TRAb are not found in some patients that have clinical manifestations, a hormone profile and imaging features highly indicative of GD.3Table 1 summarises 5 paediatric cases of this clinical presentation that has yet to be thoroughly investigated and not well understood.
Table 1.Summary of the clinical presentation, diagnostic test, treatment and outcomes of the cases.
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | |
|---|---|---|---|---|---|
| Agea | 12 years | 14 years | 10 years | 20 days | 3 years |
| Sex | F | F | F | M | F |
| Family history | Mother with GD and hypothyroidism from 2nd pregnancy | Maternal aunt with acquired hypothyroidism | Unremarkable | Mother with GD that eventually underwent thyroidectomy for MTC | Older sister and paternal aunt with hyperthyroidism |
| Personal history | Juvenile idiopathic arthritis from age 3 years | Allergy to dust mites. Mild intermittent asthma | Unremarkable | PTNB 29 weeks GA | Unremarkable |
| Neonatal sepsis, IVH, osteopenia | |||||
| Clinical featuresa | Goitre, agitation, insomnia, appetite, weight loss, hot flashes | Goitre with symptoms of hypothyroidism. Later, more severe goitre and symptoms of hyperthyroidism (insomnia, tremors, tachycardia and weight loss) | Goitre, insomnia, palpitations, agitation | Jaundice, cholestasis, tachycardia | Goitre, agitation, insomnia, tachycardia |
| TSHa (0.64-6.27 mU/L) | 0.01 | 0.426 → 0.23 | 0.01 | 0.02 | Suppressedc |
| fT4a (0.8-1.76 ng/dL) | 2.09 | 1.42 → 2.31 | 1.71 | > 7.77 | High |
| T3La (2.3-4.2 pg/mL) | 7.58 | 3.83 → 4.58 | |||
| Anti-TPOa (0-35 UI/mL) | 2.669 | 84.2 | 61 | Negativec | |
| Anti-TGa (0-40 UI/mL) | 292 | 1812 | 70 | Negativec | |
| TRAba (0-1.8 UI/mL) | < 0.3 IU/L | < 0.3 IU/L | TSIb-LATS: 5.2 (NR: 0-15 IU/L) | < 0.3 IU/L (mother and patient) | < 0.3 IU/L |
| Ultrasound | Heterogeneous | Diffusely increased thyroid blood flow on Doppler | Diffusely increased thyroid blood flow on Doppler | normal | Diffuse enlargement heterogeneous |
| Increased thyroid blood flow Doppler | |||||
| Scintigraphy | Diffuse heterogeneous mild uptake | Diffuse uptake | |||
| Treatment | Methimazole (> 1.5 years) | Propranolol (6 wk) | Methimazole | Lugol’s iodine 5 days | Methimazole (> 10 years) ± levothyroxine |
| Methimazole (> 1 year) | Levothyroxine | Levothyroxine 8 months | |||
| Radioiodine | |||||
| Current age | 14 years | 15 years | 17 years | 4 years | 13 years |
| Outcome | Resolution of symptoms and stable thyroid function with treatment | Resolution of symptoms and stable thyroid function with treatment | Poor control | Hypothyroidism secondary to Lugol’s iodine → euthyroidism | Relapses precluding discontinuation of methimazole |
| TRAb + at 3 years from onset |
The normal range applied in our laboratory is presented in parenthesis along with the corresponding units of measure.
fT4, free thyroxine; GA, gestational age; GD, gestational diabetes; IVH, intraventricular haemorrhage; MTC, medullary thyroid cancer; NR, normal range; PTNB, preterm newborn; LATS, long-acting thyroid stimulator; TG, thyroglobulin; TPO, thyroid peroxidase; TRAb, TSH Receptor Antibody; TSH, thyroid-stimulating hormone; TSI, thyroid-stimulating immunoglobulin.
aAt the time of diagnosis.
bThe method used for detection of TRAb at the time was not the same used at present.
cPatient followed up in a different hospital through age 10 years, the records provided by the patient did not include the values at diagnosis.
Case 1: pubertal patient with a personal and family history of autoimmune disease presenting with clinical hyperthyroidism with low levels of TSH and levels of free thyroxine (T4) in the upper limit of normal in successive laboratory tests in the 2 months that followed. The levels of anti-thyroid peroxidase (TPO) antibodies and anti-thyroglobulin (TG) antibodies were high, and the findings of the ultrasound examination were compatible with thyroiditis. The disease is currently controlled with antithyroid drugs.
Case 2: adolescent aged 14 years presenting with manifestations characteristic of hypothyroidism at onset: asthenia, malaise, somnolence, abdominal pain, constipation and decreased appetite. The relevant findings of blood tests were a low level of TSH with an initially normal level of free T4, with progression within a month to a presentation more characteristic of hyperthyroidism: palpitations, agitation, insomnia, palpebral retraction, goitre and elevation of free T4.
Case 3: girl aged 10 years with clinical and biochemical features compatible with hyperthyroidism. During the follow-up, the patient exhibited hypothyroidism at low doses of methimazole, leading to discontinuation of treatment after 1.5 years, upon which the patient relapsed and was finally treated with radioiodine. The TRAb detection tests were mildly positive using first-generation assays at 3 years from onset, and later became clearly positive with second-generation binding assays.
Case 4: newborn infant that developed transient neonatal hyperthyroidism with a family history of GD in the mother, who had undergone thyroidectomy for treatment of papillary thyroid cancer. The results of second-generation binding assays for detection of TRAb were negative in both mother and child.
Case 5: patient presenting with early-onset persistent hyperthyroidism with a family history of hyperthyroidism and negative TRAb results. The results of gene testing for TSHR-activating mutations were negative. The patient is scheduled to receive radioiodine for curative treatment.
Although there are few studies in the paediatric population, it appears that patients with hyperthyroidism compatible with GD and undetectable levels of TRAb exhibit thyrotoxicosis with milder clinical manifestations and biochemical abnormalities.3 In this regard, our findings were consistent with the existing literature: none of the 5 patients had thyroid eye disease or pretibial myxoedema, and the levels of free T4 at diagnosis were not very high.
In cases 2 and 3, with a mostly silent course, we could hypothesise the coexistence of TSAb and TBAb in the disease process. Recent studies have found evidence of coexistence and changes in the relative proportions of TSAb and TBAb in a single patient, mainly during pregnancy and in up to 10% of patients with GD treated with antithyroid drugs.4 For this reason, in addition to their higher sensitivity, some authors recommend using bioassays in the diagnosis of patients expected to have low antibody levels, pregnant women and cases of neonatal hyperthyroidism.2
If a patient presents with hyperthyroidism and tests negative for TRAb, the first step would be to make a differential diagnosis with the thyrotoxic phase of Hashimoto thyroiditis (ultrasound findings and compatible antibodies with a reduction in free T4 levels in a few weeks). Although they are infrequent (4.5% of patients with hyperthyroidism, diffuse goitre and negative TRAb5), in cases with early onset, a relevant family history and a poor response to antithyroid drugs (case 5), the possibility of TSHR-activating mutations should be contemplated. Other causes of thyrotoxicosis can be ruled out through the history-taking, physical examination and sonography.
Once the alternative diagnoses have been ruled out, one possible explanation to negative results of tests for detection of TRAb is that they may not be sensitive enough to detect low antibody concentrations. Another possible explanation is that the production of TRAb is restricted to the thyroid and the antibodies never enter the systemic circulation. This hypothesis is based on evidence that lymphocytes isolated from the thyroid of a patient with autoimmune thyroiditis in whom TRAb were not detected in blood could produce antithyroid autoantibodies.3,6
In conclusion, GD cannot be ruled out in patients with a clinical presentation compatible with hyperthyroidism and negative TRAb. It is important to be aware of this potential presentation in order to initiate treatment with antithyroid agents as soon as possible.
References[1]K. Stożek, A. Bossowski, K. Ziora, A. Bossowska, M. Mrugacz, A. Noczyńska, et al.Functional TSH receptor antibodies in children with autoimmune thyroid diseases.Autoimmunity., 51 (2018), pp. 62-68 http://dx.doi.org/10.1080/08916934.2018.1431776 | Medline[2]T. Diana, R.S. Brown, A. Bossowski, M Segni, M Niedziela, J Konig, et al.Clinical relevance of thyroid-stimulating autoantibodies in pediatric Graves’ disease—a multicenter study.J Clin Endocrinol Metab., 99 (2014), pp. 1648-1655 http://dx.doi.org/10.1210/jc.2013-4026 | Medline[3]X.G. Vos, N. Smit, E. Endert, J.G. Tijissen, W.M. Wiersinga.Frequency and characteristics of TBII-seronegative patients in a population with untreated Graves’ hyperthyroidism: a prospective study.Clin Endocrinol (Oxf)., 69 (2008), pp. 311-317 http://dx.doi.org/10.1111/j.1365-2265.2008.03192.x | Medline[4]S.M. McLachlan, B. Rapoport.Thyrotropin-blocking autoantibodies and thyroid-stimulating autoantibodies: potential mechanisms involved in the pendulum swinging from hypothyroidism to hyperthyroidism or vice versa.Thyroid., 23 (2013), pp. 14-24 http://dx.doi.org/10.1089/thy.2012.0374 | Medline[5]F.W. Kiefer, K. Klebermass-Schrehof, M. Steiner, C. Worda, G. Kasprian, T. Diana, et al.Fetal/neonatal thyrotoxicosis in a newborn from a hypothyroid woman with Hashimoto’s thyroiditis.J Clin Endocrinol Metab, 102 (2017), pp. 6-9 http://dx.doi.org/10.1210/jc.2016-2999 | Medline[6]M.P. Armengol, M. Juan, A. Lucas-Martín, M.T. Fernández-Figueras, D. Jaraquemada, T. Gallart, et al.Thyroid autoimmune disease: demonstration of thyroid antigen-specific b cells and recombination-activating gene expression in chemokine-containing active intrathyroidal germinal centers.Am J Pathol, 159 (2001), pp. 861-873 http://dx.doi.org/10.1016/S0002-9440(10)61762-2 | Medline ☆Please cite this article as: Scatti Regàs A, Pujol Borrell R, Ferrer Costa R, Puerto Carranza E, Clemente León M. Enfermedad de Graves con autoanticuerpos contra el receptor de la TSH negativos: a propósito de 5 casos. An Pediatr (Barc). 2020;93:417–419.
Từ khóa » Tsh à 5 4
-
Table 5-4, Agents That May Affect TSH Secretion - Endotext - NCBI
-
Các Chỉ Số Xét Nghiệm Máu đánh Giá Chức Năng Tuyến Giáp
-
Thyroid-Stimulating Hormone (TSH): TSH Levels Test - WebMD
-
The Upper Limit For TSH During Pregnancy: Why We Should Stop Using ...
-
Is There A Need To Redefine The Upper Normal Limit Of TSH? In
-
TSH-receptor Autoimmunity In Graves' Disease After Therapy With Anti ...
-
Thyroid Function Tests
-
What They're For, Plus 4 Best TSH Home Tests - Healthline
-
TSH Levels: Low To High Ranges, Symptoms, And What They Mean
-
TSH Stimulates IL-6 Secretion From Adipocytes In Culture
-
Blood Test: Thyroid Stimulating Hormone (TSH) - Kids Health
-
Thyroxine (T4) Test: MedlinePlus Medical Test
-
Macro-TSH: A Diagnostic Challenge - FullText - Karger Publishers